dddddd
By Jack Whittaker
| February 27, 2026

The CMS Access Model represents a significant shift in how Medicare reimburses healthcare providers for managing chronic conditions and specialized care. This comprehensive guide breaks down everything healthcare providers need to know about payment structures, clinical tracks, revenue calculations, and strategies to maximize reimbursements under this innovative payment model.
The Centers for Medicare & Medicaid Services (CMS) continues to evolve its approach to value-based care, and the Access Model is at the forefront of this transformation. Whether you’re a healthcare administrator, practice manager, or clinical provider, understanding the intricacies of this model is essential for optimizing your revenue cycle and delivering high-quality patient care.
What Is the CMS Access Model?
The CMS Access Model is an innovative payment and care delivery model designed to improve health outcomes for Medicare beneficiaries while controlling costs. The model focuses on several key clinical areas and introduces a unique payment structure that ties reimbursements to performance metrics and care quality.
At its core, the Access Model aims to:
- Enhance care coordination for patients with chronic conditions
- Reduce unnecessary healthcare spending through proactive management
- Improve patient outcomes through value-based care delivery
- Provide predictable revenue streams for participating providers
- Support rural healthcare providers with additional resources

The four clinical tracks under the CMS Access Model
Understanding the Clinical Tracks
The CMS Access Model encompasses four distinct clinical tracks, each targeting specific patient populations and care needs:
1. Enhanced Chronic Kidney Management (eCKM)
The eCKM track focuses on patients with advanced chronic kidney disease who are at risk of progression to end-stage renal disease. This track provides enhanced support for care coordination, patient education, and early intervention strategies.
2. Chronic Kidney Management (CKM)
The CKM track serves patients with earlier stages of chronic kidney disease, emphasizing preventive care and slowing disease progression through comprehensive management approaches.
3. Musculoskeletal (MSK)
The MSK track addresses patients with musculoskeletal conditions, providing coordinated care for conditions affecting bones, joints, and muscles. This track does not have a Follow-On tier.
4. Behavioral Health (BH)
The BH track focuses on Medicare beneficiaries with behavioral health needs, integrating mental health services with primary care to improve overall health outcomes.
Key Insight
Each clinical track has its own payment structure and tier system (Initial vs. Follow-On), allowing providers to receive different reimbursement levels based on the complexity and duration of care provided.
CMS Payment Structure: Annual Allowed Amounts
Understanding how CMS actually pays under the Access Model is crucial for healthcare providers. CMS defines annual allowed amounts per beneficiary for each clinical track and tier (Initial vs. Follow-On).
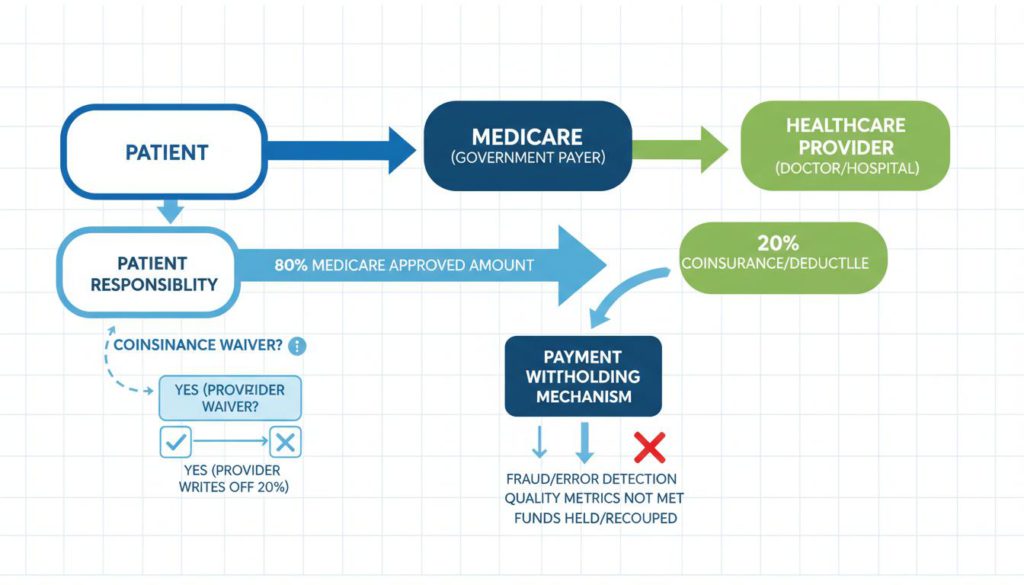
How the CMS Access Model payment flow works with the 80/20 split
Annual Allowed Amounts by Track and Tier
| Clinical Track | Initial Tier | Follow-On Tier |
|---|---|---|
| eCKM (Enhanced Chronic Kidney Management) | $360 | $180 |
| CKM (Chronic Kidney Management) | $420 | $210 |
| MSK (Musculoskeletal) | $180 | N/A (No Follow-On) |
| BH (Behavioral Health) | $180 | $90 |
Source: CMS Payment Policy Document
Understanding the 80/20 Split
CMS explains that allowed amounts include BOTH:
- Medicare program payment (80%) – Paid directly by Medicare
- Beneficiary coinsurance (20%) – Typically paid by the patient or supplemental insurance
Important Consideration
Organizations may adopt a uniform policy to waive beneficiary coinsurance consistent with model requirements. If you waive the 20% coinsurance, your collectible revenue per patient is only the Medicare 80% portion (unless supplemental payer covers the coinsurance).
Cashflow Timing: The 50/50 Split
One of the most critical aspects of the CMS Access Model is how payments are distributed over time. CMS uses a unique withholding mechanism to ensure performance accountability:
How the Payment Schedule Works
Monthly Payments
CMS issues monthly payments equal to 1/12 of the Medicare portion of the annual allowed amount.
50% In-Year Cap
The sum of monthly payments may not exceed 50% of the Medicare portion.
50% Withheld
The remaining 50% is withheld and reconciled after the 12-month care period.
Economic Breakdown
For the Medicare portion of payments:
- In-year cash received (maximum) = 50% of Medicare portion
- Withheld amount = Remaining 50% of Medicare portion
- Final total = Depends on performance adjustments
Performance Thresholds
During the effective period, CMS has established key performance thresholds:
Outcome Attainment Threshold (OAT)
OAT = 50% – This is the minimum share of aligned beneficiaries meeting all required targets to earn full payment at the organization level.
Substitute Spend Threshold (SST)
SST = 90% – Exceeding substitute spend can reduce Organization Attainment Payments (OAPs).
Detailed Per-Patient Revenue Calculations
Let’s break down the revenue calculations for each track and tier, assuming your organization waives the 20% coinsurance. This analysis shows:
- CMS Allowed Amount (100%)
- Medicare Portion (80%) = Allowed × 0.80
- Coinsurance (20%) = Allowed × 0.20 → Waived, so revenue = $0
- Maximum cash received during 12 months = Medicare × 0.50
- Maximum additional reconciliation payment (best case) = Medicare × 0.50
- Best-case total 1-year revenue = Medicare (80% of allowed)
- Worst-case floor = Medicare × 0.50 (cash already paid)
A. eCKM Track Revenue Analysis
eCKM – Initial Tier
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $360 |
| Medicare Portion (80%) | $360 × 0.80 | $288 |
| Coinsurance (20%) | $360 × 0.20 | $72 → Waived ($0) |
| In-year cash (max) | $288 × 0.50 | $144 |
| Withheld amount | $288 × 0.50 | $144 |
| Best-case 1-year revenue | Full Medicare portion | $288 |
| Worst-case floor | If none of withheld earned | $144 |
eCKM – Follow-On Tier
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $180 |
| Medicare Portion (80%) | $180 × 0.80 | $144 |
| Coinsurance (20%) | $180 × 0.20 | $36 → Waived ($0) |
| In-year cash (max) | $144 × 0.50 | $72 |
| Withheld amount | $144 × 0.50 | $72 |
| Best-case 1-year revenue | Full Medicare portion | $144 |
| Worst-case floor | If none of withheld earned | $72 |
B. CKM Track Revenue Analysis
CKM – Initial Tier
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $420 |
| Medicare Portion (80%) | $420 × 0.80 | $336 |
| Coinsurance (20%) | $420 × 0.20 | $84 → Waived ($0) |
| In-year cash (max) | $336 × 0.50 | $168 |
| Withheld amount | $336 × 0.50 | $168 |
| Best-case 1-year revenue | Full Medicare portion | $336 |
| Worst-case floor | If none of withheld earned | $168 |
CKM – Follow-On Tier
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $210 |
| Medicare Portion (80%) | $210 × 0.80 | $168 |
| Coinsurance (20%) | $210 × 0.20 | $42 → Waived ($0) |
| In-year cash (max) | $168 × 0.50 | $84 |
| Withheld amount | $168 × 0.50 | $84 |
| Best-case 1-year revenue | Full Medicare portion | $168 |
| Worst-case floor | If none of withheld earned | $84 |
C. MSK Track Revenue Analysis
The MSK track has only an Initial tier (no Follow-On tier):
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $180 |
| Medicare Portion (80%) | $180 × 0.80 | $144 |
| Coinsurance (20%) | $180 × 0.20 | $36 → Waived ($0) |
| In-year cash (max) | $144 × 0.50 | $72 |
| Withheld amount | $144 × 0.50 | $72 |
| Best-case 1-year revenue | Full Medicare portion | $144 |
| Worst-case floor | If none of withheld earned | $72 |
D. Behavioral Health (BH) Track Revenue Analysis
BH – Initial Tier
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $180 |
| Medicare Portion (80%) | $180 × 0.80 | $144 |
| Coinsurance (20%) | $180 × 0.20 | $36 → Waived ($0) |
| In-year cash (max) | $144 × 0.50 | $72 |
| Withheld amount | $144 × 0.50 | $72 |
| Best-case 1-year revenue | Full Medicare portion | $144 |
| Worst-case floor | If none of withheld earned | $72 |
BH – Follow-On Tier
| Component | Calculation | Amount |
|---|---|---|
| CMS Allowed Amount | Base amount | $90 |
| Medicare Portion (80%) | $90 × 0.80 | $72 |
| Coinsurance (20%) | $90 × 0.20 | $18 → Waived ($0) |
| In-year cash (max) | $72 × 0.50 | $36 |
| Withheld amount | $72 × 0.50 | $36 |
| Best-case 1-year revenue | Full Medicare portion | $72 |
| Worst-case floor | If none of withheld earned | $36 |
One-Year Revenue Potential Summary
The following table provides a comprehensive overview of revenue potential per patient per year, assuming coinsurance is waived:
| Track / Tier | CMS Allowed (100%) | Medicare (80%) = Your Best-Case | Coinsurance (20%) Waived | Max Cash During Year (50% of Medicare) | Withheld (50% of Medicare) |
|---|---|---|---|---|---|
| eCKM Initial | $360 | $288 | $72 | $144 | $144 |
| eCKM Follow-On | $180 | $144 | $36 | $72 | $72 |
| CKM Initial | $420 | $336 | $84 | $168 | $168 |
| CKM Follow-On | $210 | $168 | $42 | $84 | $84 |
| MSK Initial | $180 | $144 | $36 | $72 | $72 |
| BH Initial | $180 | $144 | $36 | $72 | $72 |
| BH Follow-On | $90 | $72 | $18 | $36 | $36 |
Source: CMS Payment Policy Document – Access Payments Amounts and Performance Targets
Calculating Total Annual Revenue Across Your Patient Panel
To project your organization’s total annual revenue under the CMS Access Model, you’ll need to calculate based on your patient volumes across each track and tier.
Patient Volume Variables
Let’s define the variables for your patient panel:
NeI = # of eCKM Initial patients
NeF = # of eCKM Follow-On patients
NcI = # of CKM Initial patients
NcF = # of CKM Follow-On patients
Nm = # of MSK Initial patients
NbI = # of BH Initial patients
NbF = # of BH Follow-On patientsA. Best-Case Total Annual Revenue (Coinsurance Waived)
When you waive coinsurance, your best-case revenue equals the full Medicare 80% portion:
Total Best-Case Revenue =
288(NeI) + 144(NeF) + 336(NcI) + 168(NcF) + 144(Nm) + 144(NbI) + 72(NbF)All dollar values are per patient per year, derived from CMS allowed amounts × 0.8
B. In-Year Cashflow (Upper Bound, Before Reconciliation)
Since CMS caps in-year payments at 50% of the Medicare portion:
Max Cash Received During Year =
144(NeI) + 72(NeF) + 168(NcI) + 84(NcF) + 72(Nm) + 72(NbI) + 36(NbF)The remainder is withheld pending reconciliation at the end of the care period.
C. Modeling Performance Risk (Reconciliation)
CMS ties full payment to organizational performance. A practical modeling approach is to apply a reconciliation factor (r) where r ∈ [0,1] to the withheld Medicare portion:
Total Revenue ≈ In-Year Cash + r × Withheld- r = 1.0 → Best case (earn all withheld amount)
- r = 0.0 → Worst case (earn none of the withheld amount)
- Real r → Depends on Clinical Outcome Adjustment and Substitute Spend Adjustment performance
Rural Add-On Payment

Rural healthcare providers receive additional support under the CMS Access Model
Rural healthcare providers receive additional support under the CMS Access Model
CMS recognizes the unique challenges faced by rural healthcare providers and offers an additional payment to offset device distribution and support costs.
Rural Beneficiary Add-On
For rural beneficiaries aligned to eCKM or CKM during the Initial Period, CMS provides an additional fixed payment of $15 per patient.
Incorporating Rural Add-On in Projections
To include rural add-on payments in your annual projections:
Add to your totals:
+ 15 × Nrural,eI (rural eCKM Initial patients)
+ 15 × Nrural,cI (rural CKM Initial patients) Note on Payment Structure
CMS calls this a “fixed payment” but does not explicitly state whether it is also split 80/20 in the policy document. For projection purposes, treat it as a standalone $15 add-on exactly as written.
Key Takeaways for Healthcare Providers
Understand the Split
Remember that allowed amounts include both Medicare (80%) and beneficiary coinsurance (20%). Your actual revenue depends on your coinsurance waiver policy.
Plan for Cashflow
Only 50% of Medicare payments are received during the year. The remaining 50% is withheld until reconciliation, so plan your cashflow accordingly.
Focus on Performance
Meeting the OAT (50%) and SST (90%) thresholds is critical to earning the full withheld amount. Invest in care coordination and outcome tracking.
Calculate Accurately
Use the formulas provided to project your revenue based on actual patient volumes across all tracks and tiers, including rural add-ons if applicable.
Ready to Optimize Your CMS Access Model Participation?
HealthArc provides comprehensive solutions to help healthcare providers maximize their reimbursements under value-based care models. Our platform streamlines care coordination, tracks performance metrics, and ensures you meet all CMS requirements.
Conclusion
The CMS Access Model represents a significant opportunity for healthcare providers to participate in value-based care while receiving predictable reimbursement for managing chronic conditions. By understanding the payment mechanics, clinical tracks, and performance requirements, providers can optimize their participation and maximize revenue potential.
Key success factors include:
- Accurately projecting patient volumes across all clinical tracks
- Planning for the 50/50 cashflow split during the care period
- Implementing robust care coordination to meet performance thresholds
- Tracking outcomes to ensure full reconciliation payments
- Leveraging rural add-on payments where applicable
As CMS continues to evolve its value-based care initiatives, staying informed about models like Access will be crucial for healthcare organizations seeking to thrive in the changing reimbursement landscape.
Additional Resources
For the most up-to-date information on the CMS Access Model, visit the official CMS Innovation Center website and review the Access Payments Amounts and Performance Targets document.
FAQs About CMS Access Model
Q1. What is the CMS Access Model?
The CMS Access Model is a value-based payment initiative introduced by the Centers for Medicare & Medicaid Services (CMS) to improve care quality, reduce costs, and expand access to coordinated healthcare services, especially for underserved populations.
Q2. How is the CMS Access Model different from traditional fee-for-service?
Unlike fee-for-service, which reimburses providers based on volume of services, the CMS Access Model rewards providers based on quality outcomes, care coordination, and cost efficiency.
Q3. Who is eligible to participate in the CMS Access Model?
Eligibility typically includes healthcare providers, Accountable Care Organizations (ACOs), and certain safety-net providers that meet CMS participation and reporting requirements.
Q4. What are the financial benefits of participating in the CMS Access Model?
Participants may qualify for shared savings, performance-based incentives, and improved reimbursement opportunities tied to quality and patient outcomes.
Q5. Does the CMS Access Model involve financial risk?
Yes, depending on the track selected, providers may participate in upside-only risk models or two-sided risk arrangements where they share both savings and potential losses.
Q6. What reporting requirements are involved in the CMS Access Model?
Providers must submit quality metrics, cost data, and performance reports to CMS. Accurate documentation and interoperability with EHR systems are essential for compliance.
Q7. How does the CMS Access Model improve patient care?
It promotes preventive care, care coordination, chronic disease management, and data-driven decision-making to improve outcomes and reduce hospitalizations.
Q8. Can small or independent practices participate in the CMS Access Model?
Yes. Small practices can participate independently or through partnerships such as ACOs, though they may need additional support for compliance and reporting.
Q9. What role does technology play in the CMS Access Model?
Technology such as EHR integration, remote patient monitoring (RPM), analytics platforms, and population health tools helps providers track outcomes and meet CMS performance benchmarks.
Q10. How can healthcare organizations prepare for the CMS Access Model?
Organizations should assess readiness, invest in data infrastructure, train staff on value-based care processes, optimize documentation workflows, and align financial strategies with CMS quality goals.
Jack Whittaker
Sales leader and high level Operator with a demonstrated history of working in the hospital & health care industry.




Categories
Advanced Primary Care Management→AI & Care Coordination→Behavioral Health Integration→Care Management Programs→Chronic Care Management→Digital Health & Software Solutions→General Remote Care Topics→Medication Therapy Management→Pricing & Business Strategy→Principal Care Management→Remote Patient Monitoring→Remote Therapeutic Monitoring→Transitional Care Management→
Related Blog
- February 13, 2026 | Read Time: 8 mins
CPT 99445 and 99470: Complete 2026 Guide to Short-Window RPM Billing with HealthArc
CPT 99445 and CPT 99470 are transforming how practices bill for Remote...
Learn More- January 20, 2026 | Read Time: 13 mins
The Future of Care is at Home, Driven by the Rapid Expansion of Hospital-At-Home Programs.
Healthcare is evolving. A model that brings hospital-level services directly into patients'...
Learn More- December 24, 2025 | Read Time: 7 mins
What Is Patient-Centered Care? Benefits, Key Principles, and Real-World Examples
Patient-centered care is one of the most important ideas shaping how healthcare...
Learn More